Cardiovascular diseases (CVD) account for 24.8% of all deaths in India, with an age-standardized death rate of 272 per 100,000-higher than the global average. (1) Indians develop CVD nearly a decade earlier than Western populations, with 62% of deaths occurring prematurely. Key cardiometabolic risk factors-hypertension, diabetes, and obesity-have driven a 2.3-fold rise in ischemic heart disease and stroke. (2)
CVD complications are also evident in acute settings: 20% of adults hospitalized with pneumococcal pneumonia experience heart failure, arrhythmia, or myocardial infarction. (3) Nearly 12% of patients developed heart failure within a decade of hospitalization, highlighting the prolonged cardiovascular impact of systemic infections such as pneumonia. (4)
Cardiopulmonary Overlap and Risk of Respiratory Infections in CVD
Cardiovascular and respiratory diseases frequently coexist due to shared risk factors such as smoking and systemic inflammation.(5) Symptom overlap is common-cardiac conditions like heart failure may present with respiratory features (e.g., cardiac asthma), while chronic lung disease increases right ventricular strain, predisposing to CHF. (6)
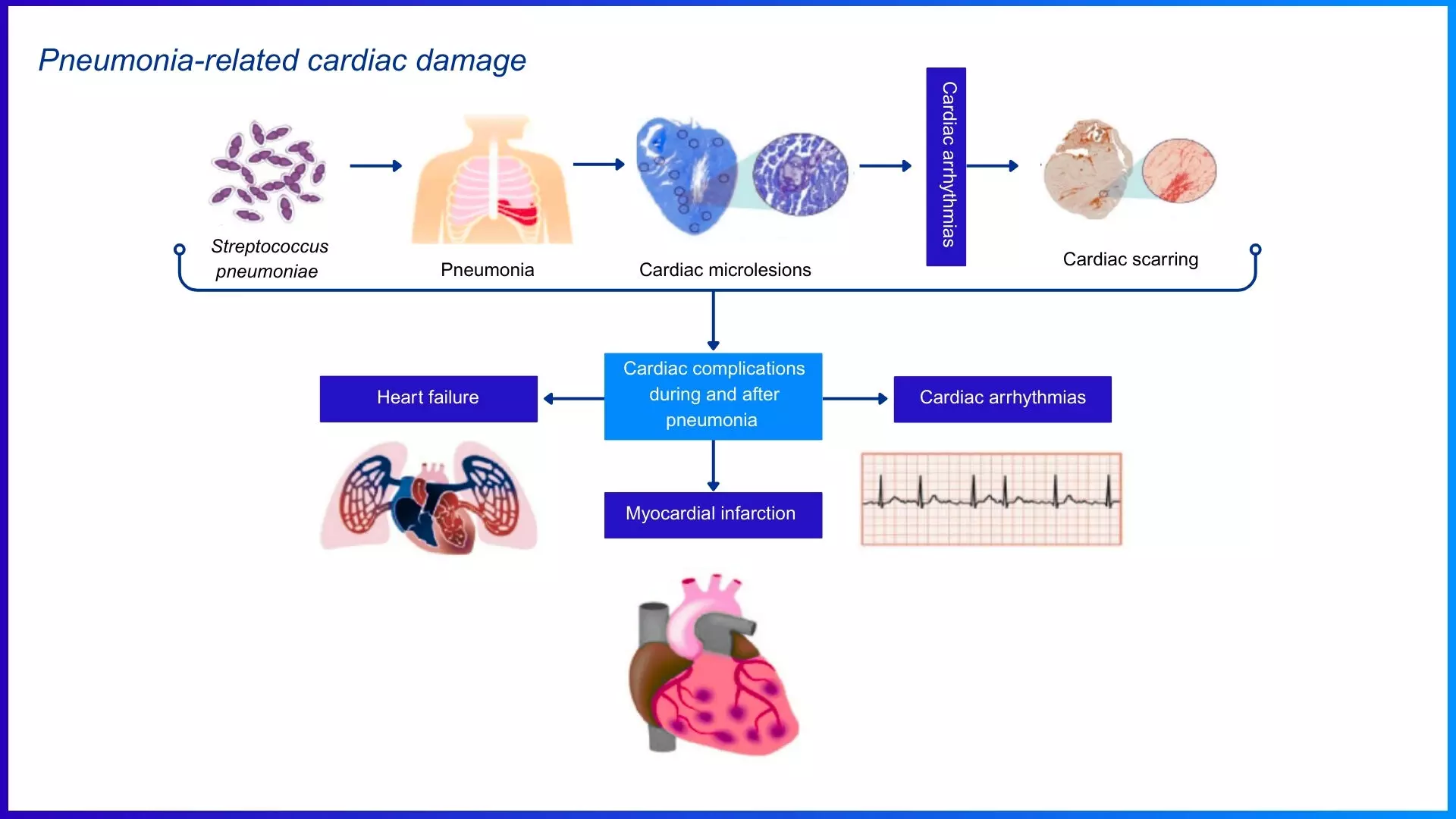
The risk intensifies with respiratory infections. Patients with cardiovascular disease—including CHF, valvular disease, and congenital heart disease—face a 3.3-fold higher risk of community-acquired pneumonia (CAP) and a 9.9-fold higher risk of invasive pneumococcal disease (IPD). (7) During IPD, Streptococcus pneumoniae translocate across the vascular endothelium and invades the myocardium, directly killing cardiomyocytes and immune cells. (8) This results in acute myocardial injury and can lead to long-term cardiac dysfunction, compounding the cardiovascular burden in affected patients. (9)
Clinical trials such as PARADIGM-HF and PARAGON-HF have demonstrated a significant incidence of pneumonia among heart failure patients. Pneumonia occurred in 6.3% (29 per 1,000 patient-years) of PARADIGM-HF patients and 10.6% (39 per 1,000 patient-years) of PARAGON-HF participants. The onset of pneumonia in these patients substantially increased the risk of adverse outcomes. (10)
Importance of Preventing Pneumococcal Disease in Cardiovascular Disease Patients
Figure: Streptococcus pneumoniae induces cardiovascular complications via multiple pathophysiological mechanisms. Adapted from Restrepo MI, Reyes LF. Respirology. 2018;23(3):250-259.
Preventing pneumococcal disease is vital for CVD patients, particularly those with heart failure and CAD, as they are more vulnerable to bacterial infections like pneumonia and other respiratory illnesses. These infections can trigger cardiac decompensation, increasing hospitalizations and mortality. Vaccination against pneumococcus lowers the risk of respiratory infections, heart failure exacerbations, and cardiovascular events. Given weakened immunity and constant exposure to airborne pathogens, vaccination helps stabilize heart function, reduce inflammation, and ease healthcare burdens. (11)
Pneumococcal Vaccination in Cardiovascular Diseases – When to Consider?
Table 1 provides adult vaccine recommendations for heart failure and related high-risk conditions per the API(Association of Physicians of India) 2024 guidelines.
Table 1: Vaccination Recommendations for High-Risk Cardiac and Chronic Conditions
|
High Risk Group
|
Recommended Vaccines
|
|
Heart Failure
|
Pneumococcal (PCV + PPSV23), Influenza (annual), COVID-19 (annual), Zoster (≥50 yrs)
|
|
Coronary Artery Disease
|
Pneumococcal, Influenza, COVID-19
|
|
Valvular / Congenital HD
|
Pneumococcal, Influenza, COVID-19
|
|
Post-Cardiac Surgery
|
Pneumococcal, Influenza, COVID-19, Hepatitis B (if high exposure risk)
|
|
CKD / Dialysis
|
Pneumococcal, Hepatitis B, Influenza, COVID-19, Tdap
|
|
Chronic Liver Disease
|
Hepatitis A, Hepatitis B, Pneumococcal, Influenza, COVID-19
|
|
T2DM
|
Pneumococcal, Influenza, Hepatitis B, COVID-19
|
|
Immunocompromised States (e.g. HIV, cancer)
|
Pneumococcal, Influenza, Hepatitis A/B, COVID-19, HPV (if age-eligible)
|
|
Age ≥50
|
Pneumococcal, Influenza, COVID-19, Zoster, Tdap
|
Vaccination should be considered a priority for individuals with CVD, as they are inherently immunocompromised due to circulatory impairment and elevated inflammatory cytokines. Advancing age (55+), diabetes, and hypertension further increase infection risk and worsen CAD. Those with congenital or valvular heart disease and post-cardiac surgery patients also face high infection risks and must adhere to vaccination protocols, particularly for pneumococcal vaccine. (12)
Pneumococcal conjugate vaccine (PCV13) should be administered first, followed by the pneumococcal polysaccharide vaccine (PPSV23) after eight weeks. (13)
Vaccination in Cardiovascular Diseases – View of Scientific Authorities
Table 2 lists vaccines with Class recommendations for adults with cardiovascular and related chronic conditions. (13)
Table 2: Approved Class I Vaccine Recommendations in High-Risk Adults
|
Vaccine
|
Class I Recommendations
|
|
Influenza
|
CVD, T2DM, lung disease, age ≥50 years, immunocompromised
|
|
Pneumococcal
|
CVD, age ≥50 years, T2DM, CKD, chronic lung disease
|
|
Tdap / Td
|
All adults every 10 years pregnancy
|
|
Hepatitis B
|
T2DM, CKD, chronic lung disease, high-risk behavior
|
|
Herpes Zoster
|
Age ≥50 years, immunocompromised, chronic heart and lung disease
|
|
COVID-19
|
Annually, all with chronic comorbidities
|
Leading health organizations strongly recommend pneumococcal and influenza vaccination for patients with chronic cardiovascular disease. The Centers for Disease Control and Prevention/Advisory Committee on Immunization Practices (CDC/ACIP) advises pneumococcal vaccination for all adults over 50 and high-risk cardiovascular patients, alongside annual influenza vaccination for those with chronic heart and lung diseases. (14) Table 3 summarizes key vaccination recommendations from major global and national health authorities.
Table 3: Pneumococcal Vaccination Recommendations by Leading Health Organizations
|
Guideline/Organization
|
Vaccine Recommendation
|
|
Indian Consensus Guidelines on Adult Immunization by the Association of Physicians of India [API, 2024] (13)
|
Recommends pneumococcal vaccines for adults aged 18-49 years with underlying conditions (chronic heart, chronic lung, diabetes, liver, kidney disease) and all adults aged 50+ years.
|
|
European Society of Cardiology [ESC, 2021] (15)
|
Suggest pneumococcal vaccination as part of heart failure management.
|
|
World Health Organization [WHO,2021] (16)
|
Advises pneumococcal vaccine for older adults.
|
|
American Heart Association [AHA, 2013] (15)
|
Suggest pneumococcal vaccination as part of heart failure management.
|
|
Heart Failure Society of America [HFSA, 2010] (11)
|
Recommends pneumococcal vaccine for all heart failure patients.
|
Additional recommended vaccines include Hepatitis B, which supports liver and overall health, and the shingles (herpes zoster) vaccine, as heart failure patients are prone to outbreaks due to stress, viral infections, and immune dysfunction.(12)
Effectiveness of Pneumococcal Vaccination in Improving Cardiovascular Outcomes
Vaccination significantly reduces hospitalizations and cardiovascular complications. A meta-analysis of 15 studies (347,444 patients) showed that pneumococcal vaccination reduced all-cause mortality by 24% (HR: 0.76, 95% CI: 0.66–0.87, p< 0.001) and myocardial infarction (MI) by 27% (HR: 0.73, 95% CI: 0.56–0.96, p = 0.02). (17) Another meta-analysis of seven studies (163,756 participants) showed pneumococcal vaccination reduced all-cause mortality by 22% (HR: 0.78, 95% CI: 0.73–0.83, p < 0.001). These findings highlight pneumococcal vaccination as a crucial preventive strategy for individuals at high cardiovascular risk, particularly those aged ≥65 years. (18)
Overcoming Barriers to Vaccination in Cardiac Patients – Multi-stakeholder Approach
Vaccine adherence remains low due to concerns about side effects, physician hesitancy, and cost. While cost is a barrier, hospitalization expenses for preventable infections are far higher. To improve adherence, public health initiatives, patient education, and enhanced accessibility are key. Effective strategies include patient messaging and community education to emphasize vaccines as essential for reducing cardiovascular risk and improving long-term health. (19)
Take Home Message
- CVD causes 24.8% of all deaths in India, with earlier onset and high premature mortality-highlighting the need to reduce preventable complications and secondary risks.
- Patients with CVD face a 3.3-fold higher risk of pneumonia and a 9.9-fold higher risk of invasive pneumococcal disease, which can cause acute and long-term myocardial damage.
- Pneumococcal vaccination lowers all-cause mortality by up to 24% and reduces myocardial infarction risk by 27%, supporting its role in cardiovascular risk reduction.
- API recommends pneumococcal vaccination for adults aged 18–49 with comorbidities, including chronic heart disease, and for all adults aged above 50.
- Despite strong endorsements from CDC, AHA, ESC, and Indian consensus guidelines, vaccine uptake in cardiac patients remains low-necessitating targeted education and public health action.
References:
1. Jan, Bisma et al. “Cardiovascular Diseases Among Indian Older Adults: A Comprehensive Review.” Cardiovascular therapeutics vol. 2024 6894693. 25 Jun. 2024.
2. Kalra, Ankur et al. “The burgeoning cardiovascular disease epidemic in Indians – perspectives on contextual factors and potential solutions.” The Lancet regional health. Southeast Asia vol. 12 100156. 10 Feb. 2023, doi:10.1016/j.lansea.2023.100156
3. Musher, Daniel M et al. “The association between pneumococcal pneumonia and acute cardiac events.” Clinical infectious diseases : an official publication of the Infectious Diseases Society of America vol. 45,2 (2007): 158-65. doi:10.1086/518849
4. Eurich, Dean T et al. “Risk of heart failure after community acquired pneumonia: prospective controlled study with 10 years of follow-up.” BMJ (Clinical research ed.) vol. 356 j413. 13 Feb. 2017, doi:10.1136/bmj.j413
5. Carter, Paul et al. “Association of Cardiovascular Disease With Respiratory Disease.” Journal of the American College of Cardiology vol. 73,17 (2019): 2166-2177. doi:10.1016/j.jacc.2018.11.063
6. Buckner, Kern. “Cardiac asthma.” Immunology and allergy clinics of North America vol. 33,1 (2013): 35-44. doi:10.1016/j.iac.2012.10.012
7. Torres, Antoni et al. “Which individuals are at increased risk of pneumococcal disease and why? Impact of COPD, asthma, smoking, diabetes, and/or chronic heart disease on community-acquired pneumonia and invasive pneumococcal disease.” Thorax vol. 70,10 (2015): 984-9. doi:10.1136/thoraxjnl-2015-206780
8. Brown, Armand O et al. “Streptococcus pneumoniae translocates into the myocardium and forms unique microlesions that disrupt cardiac function.” PLoS pathogens vol. 10,9 e1004383. 18 Sep. 2014, doi:10.1371/journal.ppat.1004383
9. Shenoy, Anukul T et al. “Streptococcus pneumoniae in the heart subvert the host response through biofilm-mediated resident macrophage killing.” PLoS pathogens vol. 13,8 e1006582. 25 Aug. 2017, doi:10.1371/journal.ppat.1006582
10. Shen L, Jhund PS, Anand IS, et al. Incidence and Outcomes of Pneumonia in Patients With Heart Failure. J Am Coll Cardiol. 2021;77(16):1961-1973.
11. Bhatt AS, DeVore AD, Hernandez AF, Mentz RJ. Can Vaccinations Improve Heart Failure Outcomes?: Contemporary Data and Future Directions. JACC Heart Fail. 2017;5(3):194-203.
12. Centers for Disease Control and Prevention. “Vaccination Information for Adults with Heart Disease.” CDC, https://www.cdc.gov/vaccines/adults/rec-vac/heart-disease-home.html. Accessed 19 Feb. 2025.
13. Indian Consensus Guideline on Adult Immunization.EMVAC, June 2024, https://www.emvac.in/wp-content/uploads/2024/06/Adult-Vaccination-Booklet.pdf. Accessed 25 Feb. 2025.
14. U.S. Centers for Disease Control and Prevention.CDC Recommends Lowering the Age for Pneumococcal Vaccination from 65 to 50 Years Old. Accessed on 2nd January 2025 from https://www.cdc.gov/media/releases/2024/s1023-pneumococcal-vaccination.html
15. Jaiswal V, Ang SP, Lnu K, et al. Effect of Pneumococcal Vaccine on Mortality and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis. J Clin Med. 2022;11(13):3799. Published 2022 Jun 30. doi:10.3390/jcm11133799
16. World Health Organization. (n.d.). Pneumonia. Immunization, Vaccines and Biologicals. Retrieved from https://www.who.int/
17. Jaiswal V, Ang SP, Lnu K, et al. Effect of Pneumococcal Vaccine on Mortality and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis. J Clin Med. 2022;11(13):3799. Published 2022 Jun 30.
18. Marques Antunes M, Duarte GS, Brito D, et al. Pneumococcal vaccination in adults at very high risk or with established cardiovascular disease: systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes. 2021;7(1):97-106.
19. García-Zamora S, Pulido L. Vaccines in cardiology, an underutilized strategy to reduce the residual cardiovascular risk. Arch Peru Cardiol Cir Cardiovasc. 2024;5(1):29-39. Published 2024 Mar 19.