Nighttime acid reflux commonly referred to as nocturnal acid breakthrough (NAB) is defined as a persistent decrease in intragastric pH below 4 for more than 60 minutes at night. (1) It has clinical sequels, particularly in patients with complicated gastroesophageal reflux disease (GERD), Barrett’s esophagus, and esophageal motility abnormalities. (2) Nocturnal acid breakthrough (NAB) occurs in 40% to 70% of patients with GERD who are being treated with proton pump inhibitors (PPIs), (1) and more than 70% of Helicobacter pylori-negative patients on PPI therapy. (2)
Clinical Relevance of Nocturnal Acid Breakthrough
Most individuals are recumbent during nighttime and do not swallow as frequently as during daytime. Without the assistance of gravity and with decreased salivary buffering, esophageal acid clearance depends primarily on esophageal peristalsis. Therefore, a nocturnal acid breakthrough is particularly relevant in patients with complicated GERD, Barrett’s esophagus, and esophageal motility abnormalities. (2)
Interestingly, clinical studies have indicated that nocturnal acid breakthrough is an isolated gastric phenomenon and esophageal acid suppression, and symptom control are not dependent on the degree of nocturnal acid breakthrough elimination. Nocturnal acid breakthrough increases the likelihood of reflux during the gastric acid breakthrough in patients with decreased lower esophageal sphincter pressure and ineffective esophageal motility, i.e. high frequency of distal esophageal body contractions <30 mmHg. (2)
Approach to Management of Nocturnal Acid Breakthrough
The maximal benefit from PPI therapy is achieved when PPIs are taken 15–30 minutes before meals, allowing optimal blood concentrations of the drug during meal-induced activation of proton pumps to produce blockade of many pumps. Researchers have also focused on eliminating NAB by targeting the histamine surge during nighttime using histamine H2 receptor antagonists (H2RA) such as ranitidine. (1) Normally, there is no food ingestion during nighttime, so bedtime dosing of H2RAs benefits inhibiting nocturnal acid secretion. Adding bedtime H2RAs is clinically effective in controlling nocturnal acid breakthrough and GERD symptoms. (2)
Examining the Evidence: Efficacy of Ranitidine in Nocturnal Acid Breakthrough
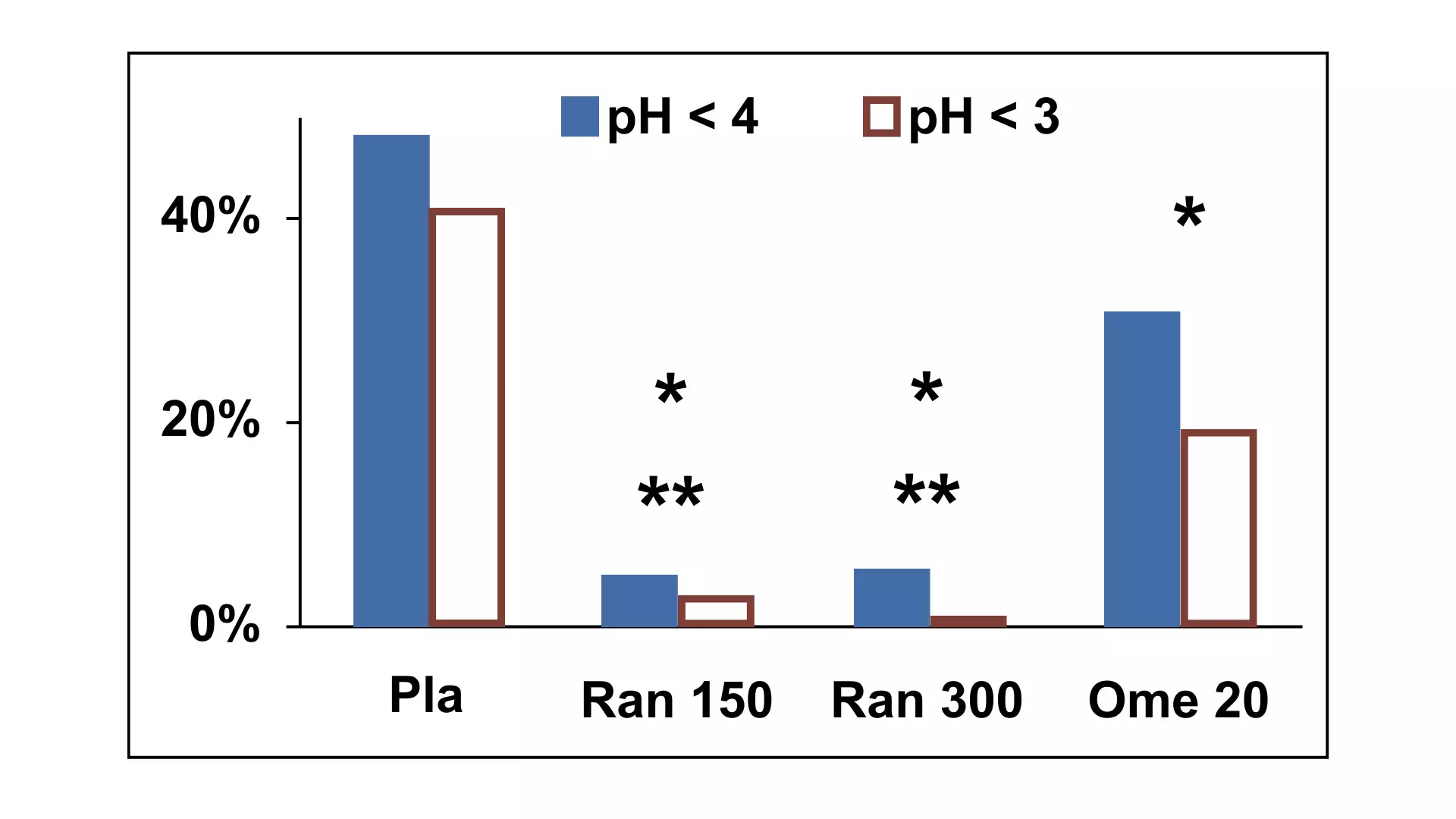
Bedtime ranitidine more effective than bedtime proton pump inhibitor (PPI): A double-blind, placebo-controlled, crossover study compared the effect of overnight intragastric pH of 20 mg omeprazole twice daily plus 20 mg at bedtime with those of 20 mg omeprazole twice daily plus 150 or 300 mg ranitidine or placebo at bedtime. The study included 12 subjects with an intragastric pH <4 for 48% of them (IQR, 35%–63%) of the overnight period with omeprazole, 20 mg twice daily, plus placebo at bedtime. A third dose of omeprazole at bedtime decreased this percentage to 31% (7%–36%; P<0.005). The result further showed that bedtime ranitidine significantly reduced the percentage of time with intragastric pH <4 by 5% with 150 mg and 6% with 300 mg (P <0.01 vs. omeprazole twice daily plus bedtime). These were significantly lower than those with placebo (p<0.001) or additional omeprazole at bedtime (p<0.01). This concludes that bedtime ranitidine is more effective than bedtime proton pump inhibitors in reducing NAB. (3)
The 4 treatments were placebo (Pla), 150 mg ranitidine (Ran 150), 300 mg ranitidine (Ran 300), and 20 mg omeprazole (Ome 20) in addition to 20 mg omeprazole twice daily. *P < 0.005 vs. placebo, **P < 0.01 vs. omeprazole 20 for both pH 4 and pH 3.
Combination of H2RAs and PPI Effective in NAB: Given the role of histamine in the nocturnal acid breakthrough mechanism, combining ranitidine at bedtime with daily PPI therapy is another effective approach to reducing nocturnal acid breakthrough. (4)
- Adding a bedtime H2RA reduces the NAB: A retrospective analysis compared the incidence of NAB with twice daily PPI with or without an H2RA. Multichannel intraluminal impedance-pH studies in 100 patients were reviewed. Fifty-eight patients (females, 41; mean age, 54 years; range, 17 to 85) were studied on twice daily PPI. Forty-two patients (females, 36; mean age, 53 years; range 20 to 85) were studied on a PPI twice daily + H2RA (Ranitidine) for at least one month at bedtime. In the patients with PPI twice daily, 64% had NAB, compared with only 17% of patients on PPI twice daily and H2RA (P<0.001). This concludes that adding a bedtime ranitidine reduces the NAB. (5)
- Bedtime ranitidine with PPI improves NAB: Another retrospective study assessed the effects of adding bedtime H2-blocker to PPI twice daily on intragastric pH control and the frequency of NAB and its effects on nocturnal esophageal reflux in GERD patients. The study divided the patients into three groups: Group A (N=60, omeprazole 20mg or lansoprazole 30mg twice daily), Group B [N=45, omeprazole 20mg or lansoprazole 30mg twice daily plus bedtime H2RA (ranitidine 300mg)] and Group C (N=11, evaluated during treatment with both regimens). The result showed that the median percentage of time with intragastric pH >4 overnight was 51% in group A, compared to 96% in group B (P<0.0001). The median percentage of time with pH >4 during the daytime was 73% in group A and 79.8% in group B (P=0.14). In group C patients, the median percentage of time with intragastric pH >4 overnight increased from 54.6% without H2RA to 96.5% after adding bedtime H2RA (P=0.0013). NAB occurred in 82% of patients in group A and 40% in group B (P<0.0001). This concludes that adding bedtime ranitidine enhances nocturnal acid breakthrough control compared to PPI. (6)
Review of Guideline Recommendations:
Indian Guideline: The Consensus Guidelines for Management of Gastroesophageal Reflux Disease by the Indian Society of Gastroenterology (ISG) and Association of Physicians of India (API) recommended adding bedtime H2RA in patients having nocturnal reflux symptoms despite the use of PPI. (Level of evidence: II-3 Grade of recommendation C) The consensus noted that adding bedtime H2RA (alone or in combination with PPI) to double dose PPI in patients with GERD decreases gastric acidity and NAB. (7)
Global Guidelines: The Seoul Consensus on the Diagnosis and Management of Gastroesophageal Reflux Disease also suggested adding the administration of H2RAs at bedtime to prevent NAB. It further noted the potential preventive role of H2RAs on nocturnal histamine-driven gastric acid secretion, supporting H2RAs as an option for patients with incomplete control of nighttime symptoms despite optimal PPI use. (8)
The Evidence-based Clinical Practice Guidelines for GERD by the Japanese Society of Gastroenterology suggested the addition of an H2RA before bedtime with a PPI to reduce NAB. (9)
Similarly, “A Management Update on the Refractory Gastroesophageal Reflux Disease” also suggested adding H2RAs at bedtime is considered to reduce and control NAB better and effectively. (10)
Key Points
- Nocturnal acid breakthrough (NAB) is the persistent decrease in intra-gastric pH below 4 for more than 60 minutes at night.
- NAB occurs in 40% to 70% of patients with GERD and more than 70% of Helicobacter pylori-negative treated with proton pump inhibitors (PPIs).
- Studies over the years suggest bedtime H2RAs, including ranitidine, are more effective than bedtime proton pump inhibitors.
- Bedtime ranitidine dosing benefits inhibiting nocturnal acid secretion, and it is comparatively more effective than PPI in reducing NAB. Adding ranitidine to a normal PPI regimen is also effective in controlling NAB incidences.
- Multiple guidelines, including Consensus Guidelines for Management of Gastroesophageal Reflux Disease by the Indian Society of Gastroenterology (ISG) and Association of Physicians of India (API) and Asian guidelines (Japanese Society of Gastroenterology and Seoul Consensus) suggested the use of bedtime ranitidine to reduce NAB.
References:
1. Jeon HK, Kim GH. Can Nocturnal Acid-breakthrough Be Reduced by Long-acting Proton Pump Inhibitors? J Neurogastroenterol Motil. 2017 Apr 30;23(2):145-148. doi: 10.5056/jnm17037.
2. Tutuian R, Castell DO. Nocturnal acid breakthrough – approach to management. MedGenMed. 2004 Oct 26;6(4):11.
3. Peghini PL, Katz PO, Castell DO. Ranitidine controls nocturnal gastric acid breakthrough on omeprazole: a controlled study in normal subjects. Gastroenterology. 1998 Dec;115(6):1335-9. doi: 10.1016/s0016-5085(98)70010-1.
4. Gerson LB, Fass R. A systematic review of the definitions, prevalence, and response to treatment of nocturnal gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2009 Apr;7(4):372-8; quiz 367. doi: 10.1016/j.cgh.2008.11.021. Epub 2008 Dec 3.
5. Mainie I, Tutuian R, Castell DO. Addition of a H2 receptor antagonist to PPI improves acid control and decreases nocturnal acid breakthrough. J Clin Gastroenterol. 2008 Jul;42(6):676-9. doi: 10.1097/MCG.0b013e31814a4e5c.
6. Xue, S., Katz, P. O., Banerjee, P., Tutuian, R., & Castell, D. O. (2001). Bedtime H2 blockers improve nocturnal gastric acid control in GERD patients on proton pump inhibitors: PROTON PUMP INHIBITORS PLUS H2RA IN GERD. Alimentary Pharmacology & Therapeutics, 15(9), 1351–1356.
7. Bhatia, Shobna et al. “API-ISG Consensus Guidelines for Management of Gastrooesophageal Reflux Disease.” The Journal of the Association of Physicians of India vol. 68,10 (2020): 69-80.
8. Jung HK, Tae CH, Song KH, Kang SJ, Park JK, Gong EJ, Shin JE, Lim HC, Lee SK, Jung DH, Choi YJ, Seo SI, Kim JS, Lee JM, Kim BJ, Kang SH, Park CH, Choi SC, Kwon JG, Park KS, Park MI, Lee TH, Kim SY, Cho YS, Lee HH, Jung KW, Kim DH, Moon HS, Miwa H, Chen CL, Gonlachanvit S, Ghoshal UC, Wu JCY, Siah KTH, Hou X, Oshima T, Choi MY, Lee KJ; Korean Society of Neurogastroenterology and Motility. 2020 Seoul Consensus on the Diagnosis and Management of Gastroesophageal Reflux Disease. J Neurogastroenterol Motil. 2021 Oct 30;27(4):453-481. doi: 10.5056/jnm21077.
9. Iwakiri K, Kinoshita Y, Habu Y, Oshima T, Manabe N, Fujiwara Y, Nagahara A, Kawamura O, Iwakiri R, Ozawa S, Ashida K, Ohara S, Kashiwagi H, Adachi K, Higuchi K, Miwa H, Fujimoto K, Kusano M, Hoshihara Y, Kawano T, Haruma K, Hongo M, Sugano K, Watanabe M, Shimosegawa T. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2015. J Gastroenterol. 2016 Aug;51(8):751-67. doi: 10.1007/s00535-016-1227-8. Epub 2016 Jun 21.
10. Rettura, Francesco et al. “Refractory Gastroesophageal Reflux Disease: A Management Update.” Frontiers in medicine vol. 8 765061. 1 Nov. 2021, doi:10.3389/fmed.2021.765061