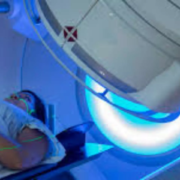
Radiation therapy could be an underused tool to reduce pelvic relapse risk for patients with locally advanced, muscle-invasive bladder cancer, according to results of a new phase III randomized trial. In the study, moderate doses of radiation therapy after bladder removal surgery sharply cut the rates of cancer returning in the pelvis without adding serious side effects. Findings of the Bladder Adjuvant RadioTherapy (BART) trial conducted at centers across India will be presented today at the American Society for Radiation Oncology (ASTRO) Annual Meeting.
“This is one of the first studies and the largest randomized trial to show that post-operative radiation therapy can meaningfully reduce pelvic relapses in bladder cancer,” said Vedang Murthy, MD, principal investigator of the trial and a professor and radiation oncologist at Tata Memorial Hospital in Mumbai. “Pelvic relapse can be devastating for patients – extremely painful and almost impossible to treat. Our research shows that modern radiation therapy offers a safe way to prevent many of these recurrences and improve patients’ quality of life.”
Locally advanced, muscle-invasive bladder cancer occurs when a tumor grows beyond the inner urothelial lining of the bladder into its muscle wall. Each year, roughly 20,000 to 25,000 people in the U.S. and more than half a million worldwide are diagnosed with muscle-invasive disease. Standard treatment for these patients typically involves radical cystectomy – surgical removal of the bladder – and chemotherapy, but up to one-third develop new pelvic tumors within two to three years.
Dr. Murthy and colleagues previously reported findings showing that adding intensity-modulated radiation therapy (IMRT) after cystectomy for patients with high-risk, muscle-invasive bladder cancer was safe and caused minimal side effects. The new analysis evaluated whether post-operative radiation therapy could also reduce cancer recurrence in the surgical bed and surrounding pelvic region.
The BART trial enrolled 153 patients with locally advanced, urothelial muscle-invasive bladder cancer from 2016 to 2024. Participants were randomly assigned to receive either post-operative/adjuvant radiation therapy (50.4 Gy in 28 fractions, n=77) or observation alone (n=76). All patients underwent radical cystectomy, and nearly all also received chemotherapy before (71%) or after (20%) surgery.
The people who enrolled in the trial were at high risk for recurrence: 62% had tumors that extended outside the bladder wall (pT3–T4), 41% had lymph node involvement (pN+), and 28% displayed variant tumor subtypes.
Patients who received radiation therapy after surgery experienced significantly fewer pelvic recurrences. Over a median follow-up of 47 months, 8% of patients in the radiation group experienced a locoregional recurrence, compared to 26% of those in the observation group (p=0.006). Two-year locoregional recurrence-free survival, the study’s primary endpoint, was 91.2% with radiation therapy versus 76.4% without (p=0.004).
“Bladder cancer is aggressive, and surgery and chemotherapy alone are not enough to prevent pelvic recurrence,” said Dr. Murthy. “But in our trial, very few people who received radiation had a locoregional relapse within two years.”
Disease-free survival (DFS), which measures time to recurrence anywhere in the body, also favored the radiation arm (77.6% vs. 64.4%, p=0.07). But rates of distant metastases were similar in both groups, affecting nearly one third of patients and reflecting the systemic nature of this cancer. Most people diagnosed with muscle-invasive bladder cancer ultimately die from distant metastases, explained Dr. Murthy, “but it does not matter where the cancer returns – whatever relapse we can reduce, we must reduce.”
Two-year overall survival was higher in the radiation arm (68% vs. 57%), though the difference was not statistically significant (p=0.4), which Dr. Murthy attributed to the small sample size. He said the next step for his team is a prospective meta-analysis combining BART data with large, randomized trials from France and Egypt to further assess safety and benefit in survival outcomes.
Side effect rates were low and similar between the groups. Severe late side effects were experienced by 8.5% of patients in the radiation arm and 10.5% in the observation arm (p=0.6). Subgroup analyses also suggested an additional benefit of radiation for patients with larger tumors (T3-4) and node-positive disease, pointing to potential directions for personalized bladder cancer treatment.
Dr. Murthy said he hopes these results will spur greater use of radiation therapy for bladder cancer. ”BART shows that modern radiation techniques allow us to deliver highly targeted treatment with fewer complications than in the past. Radiation therapy is already used safely after surgery for gynecologic cancers in the same anatomically complex region, suggesting it could also become a standard option for high-risk bladder cancer following cystectomy,” he said.
He noted that a limitation of the study is that no patients received immunotherapy, which is becoming standard in bladder cancer treatment to improve survival. Recent advances in immunotherapy highlight “a clear need” to study its use alongside post-operative radiation for patients with high-risk disease, said Dr. Murthy. “The two treatments act differently, with distinct functions and side effect profiles, and there’s no reason we shouldn’t be combining them,” he said.
Reference:
Radiation therapy after surgery safely reduces pelvic relapse risk from locally advanced, muscle-invasive bladder cancer, American Society for Radiation Oncology, Meeting: American Society for Radiation Oncology (ASTRO) 2025Annual Meeting.