Cervical fibroid: A diagnostic dilemma and operative challenge reports year long study

Uterine fibroids are the most common benign smooth muscle
tumour in women of the reproductive age group. Despite having a fairly high
frequency of 70%, uterine fibroid only impacts 20–40% of females
symptomatically. Ninety-five percent of leiomyomas are found in the uterine
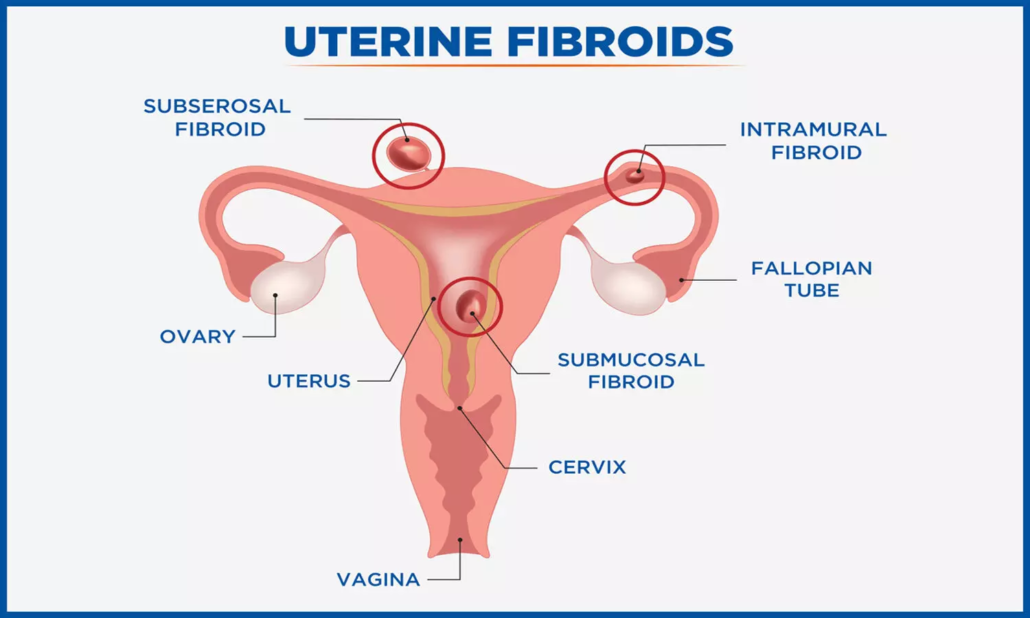
corpus; just one to two percent are seen in the cervicalregion. These tumours
are estrogen-dependent. The cervical fibroid can arise either from the
supravaginal or infravaginal portion of the cervix. It may originate from the
anterior, posterior, central, or lateral regions. Cervical fibroid is classified
as type 8 in the FIGO classification of uterine fibroid. Cervical fibroid may
be present with varied symptoms like irregular vaginal bleeding, heavy
menstrual bleeding, dysmenorrhea, chronic pelvic pain, and pressure effects
caused disturbance in bladder and bowel habits. Cervical leiomyoma can change
the shape of the cervix and cause its lengthening and effacement. It can also
cause the uterus to push upwards or the bladder to be drawn up when its size
increases, which causes urinary tract infections.
Cervical fibroid may have an impact on a woman’s obstetric
outcomes because it can result in abortion, infertility, early discomfort, more
surgical intervention, and a protracted postpartum recovery. Sometimes it is
difficult to reach the diagnosis of cervical fibroid as it mimics various other
gynaecological conditions or because of some atypical presentation like
polypoidal vaginal mass, incarcerated procidentia, chronic uterine inversion,
uterocervical descent, ovarian mass, acute urinary retention, or cervical
carcinoma. This study aimed to find out how common cervical fibroids are among
different ages, where they start, the most common symptom that led women to the
hospital, as well as any site-specific symptoms. It also was to find out if
there is a link between size and symptoms, surgical problems, and the development
of cancer. How to differentiate it from the other gynaecological entities
mentioned above? What are modalities that help in diagnosis and rule out
malignancies?
A two-year retrospective analysis of women diagnosed with
cervical leiomyoma was conducted at Obstetrics and Gynaecology department,
PGIMS Rohtak (a tertiary care institute in Northern India). A total of 24 cases
diagnosed with cervical fibroid (CF) were studied.
75% of the females had vaginal bleeding, 44.6% had heavy
menstrual bleeding, 33.3% had irregular bleeding, and one had postmenopausal
bleeding. 41.6% had urinary symptoms; 1.5% complained of vaginal discharge;
difficulty in stools (16.6%); and leiomyosarcoma (8.3%). It was discovered that
the development of malignancy and bladder and intestinal problems was linked to
an increase in CF mass, while severe anaemia and vaginal bleeding were not.
Cervical fibroid is mostly benign, can be present at
extremes of age, and its atypical presenting symptoms pose difficulty in
diagnosis. Vaginal bleeding and retention of urine are the most common
symptoms. Central and supravaginal fibroids are difficult to operate. Authors
cannot find a clear demarcation of presenting symptoms between the anterior and
posterior fibroids. Preoperative clinical evaluation, radiological imaging, and
proper intraoperative delineation of pelvic anatomy can help in their
successful management and anticipating intraoperative complications.
Intracapsular enucleation is the best approach to preventing
ureteric injury. Its management is still a challenge for gynaecologists, as
they are difficult to operate due to their proximity to the pelvic structure.
In large cervical firoids, always suspect malignancy before moving to surgery,
and hidden cervical malignancy can coexist.
Source: Dahiya et al. / Indian Journal of Obstetrics and
Gynecology Research 2024;11(3):409–414
https://doi.org/10.18231/j.ijogr.2024.074

